The clinical determination of Katherine Short’s cause of death—acute pancreatitis—shifts the narrative from tabloid speculation to a case study in rapid physiological collapse. To understand the gravity of this diagnosis, one must move beyond the superficial headline and analyze the systemic failure of the exocrine pancreas. Acute pancreatitis is not merely an "inflammation"; it is a state of biological autodigestion where the organ’s own digestive enzymes become prematurely active, effectively consuming host tissue and triggering a systemic inflammatory response syndrome (SIRS).
The Mechanism of Pancreatic Autodigestion
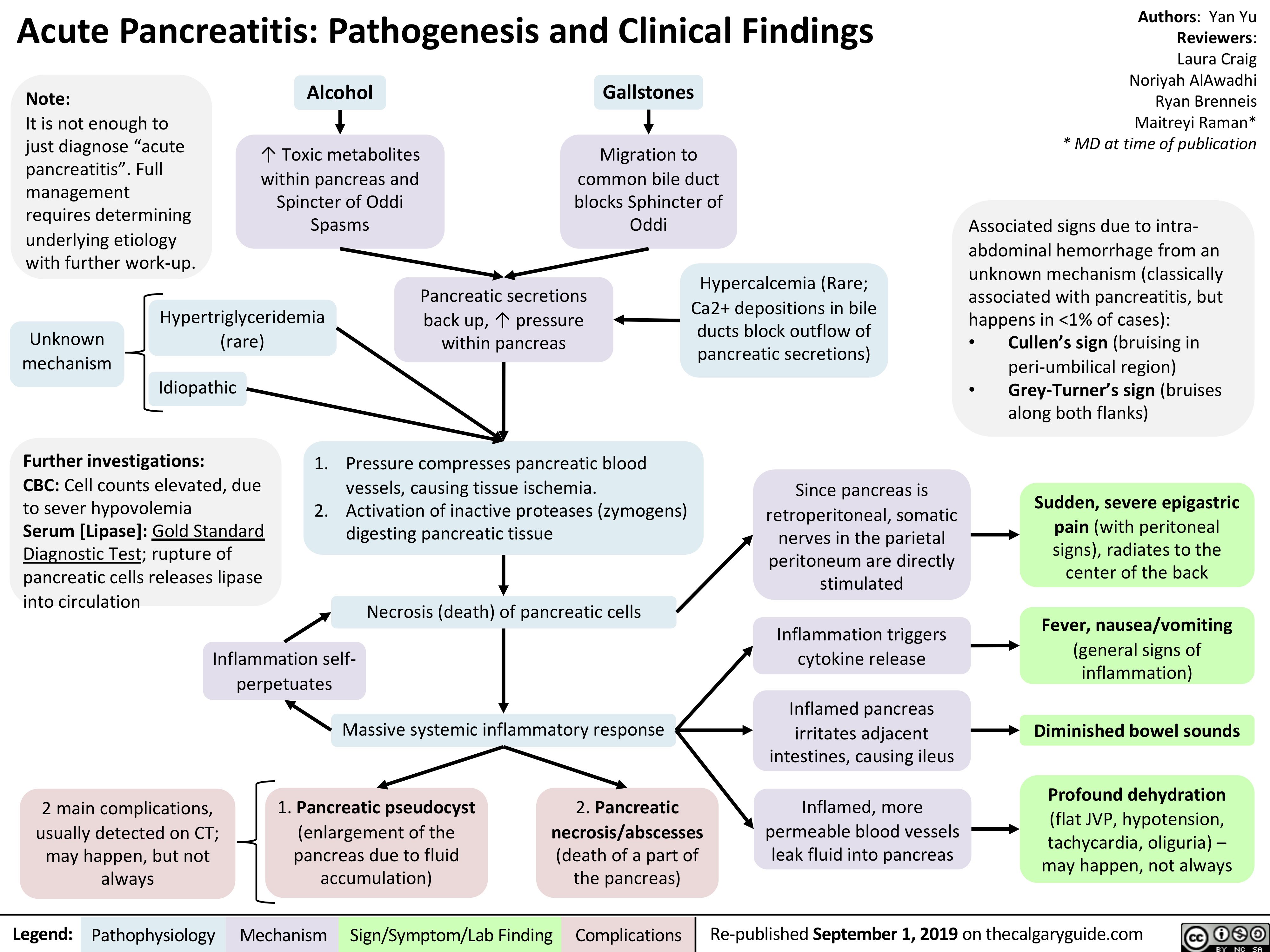
The pancreas operates on a strict compartmentalization protocol. Under normal homeostatic conditions, proenzymes (zymogens) like trypsinogen are transported to the duodenum before being converted into their active forms. In the case of acute pancreatitis, this protocol fails.
- Intracellular Activation: The premature conversion of trypsinogen to trypsin occurs within the pancreatic acinar cells.
- The Proteolytic Cascade: Once trypsin is active, it triggers a chain reaction, activating other enzymes such as elastase and phospholipase $A_2$.
- Vascular and Tissue Destruction: Elastase dissolves the elastic fibers of blood vessels, leading to hemorrhage, while phospholipase $A_2$ destroys cell membranes, resulting in localized necrosis.
The speed of this progression determines the clinical outcome. In "mild" cases, the inflammation is interstitial and edematous. In the "severe" category—which appears to be the trajectory in this instance—the pathology becomes necrotizing. This involves the death of pancreatic parenchyma and surrounding peripancreatic fat, which creates a high-risk environment for multi-organ failure.
Diagnostic Benchmarks and the "Silent" Progression
The challenge in managing pancreatic distress in high-profile or high-stress individuals often lies in the ambiguity of early symptomatic presentation. While the media focuses on the tragic outcome, the underlying clinical markers provide a more rigorous map of the event.
- Serum Amylase and Lipase Levels: A diagnostic threshold typically requires these enzymes to be at least three times the upper limit of normal. Lipase is the more specific biomarker due to its longer half-life and higher concentration within the pancreas.
- Imaging Limitations: Early-stage CT scans can occasionally yield false negatives if the inflammatory response has not yet resulted in visible structural changes or fluid collection.
- The Pain Profile: The hallmark symptom is epigastric pain radiating to the back. However, the intensity of the pain does not always correlate linearly with the severity of the tissue damage.
The "Goldilocks Zone" for intervention is exceptionally narrow. If the inflammatory mediators—specifically cytokines like $TNF-\alpha$ and $IL-6$—breach the systemic barrier, the patient enters a state of vasodilation and increased capillary permeability. This leads to third-spacing, where fluid leaks out of the circulatory system and into the interstitial space, causing a drop in blood pressure and subsequent renal or pulmonary failure.
Risk Factors and Statistical Precedents
Analyzing the cause of death requires a cold look at the statistical drivers of the condition. While the specific personal medical history of Katherine Short remains private, the epidemiological data on acute pancreatitis highlights three primary drivers:
- Biliary Obstruction: Gallstones migrating into the common bile duct, obstructing the pancreatic duct and causing back-pressure.
- Metabolic Insults: Hypertriglyceridemia or chronic ethanol consumption, both of which stress the acinar cells.
- Idiopathic Factors: Roughly 20% of cases have no identifiable external trigger, suggesting a genetic or micro-vascular predisposition.
The mortality rate for severe necrotizing pancreatitis can reach 30% even with modern intensive care. The primary cause of death in the first week is typically systemic inflammatory response leading to organ failure, whereas deaths occurring after two weeks are usually the result of infected necrosis and sepsis.
The Systemic Impact of Pancreatic Enzyme Leakage
When the pancreatic barrier is compromised, the enzymes do not remain localized. The systemic circulation carries these proteins to distant organs, creating a secondary "cascade of failure."
- Pulmonary: Phospholipases can damage lung surfactant, leading to Acute Respiratory Distress Syndrome (ARDS).
- Renal: Hypovolemia and the toxic effects of inflammatory debris often lead to acute kidney injury (AKI).
- Cardiac: Myocardial depressant factors released during the necrotic process can impair heart function, further complicating the hemodynamic stability of the patient.
The management of such a crisis requires aggressive fluid resuscitation and constant monitoring of the "Ranson Criteria" or the "APACHE II Score"—standardized metrics used by clinicians to predict the severity and mortality risk of the episode.
Strategic Medical Literacy for High-Stress Demographics
The death of Katherine Short underscores a critical gap in public health literacy regarding "internal" emergencies. Unlike cardiac events which have gained widespread awareness through "chest pain" protocols, pancreatic distress is often misidentified as severe indigestion or viral gastroenteritis until the systemic inflammatory response is already underway.
The immediate strategic priority for individuals in high-pressure environments—where stress and dietary irregularities can mask metabolic dysfunction—is the adoption of a "Zero-Threshold" policy for epigastric pain.
- Immediate Bio-Marker Testing: At the onset of unexplained abdominal radiating pain, a stat lipase test is the only reliable way to rule out pancreatic involvement.
- Hydration as a Prophylactic: Since many cases of pancreatitis are exacerbated by hemoconcentration (thickened blood), maintaining aggressive hydration levels can theoretically mitigate the severity of an early-stage inflammatory event.
- Genetic Screening: For families with a history of digestive disorders, screening for mutations in the $SPINK1$ or $PRSS1$ genes can identify a predisposition to hereditary pancreatitis, allowing for lifestyle adjustments before an acute event occurs.
The definitive forecast for this medical sector points toward an increased reliance on early-intervention enzymatic inhibitors and more sophisticated imaging. For now, the loss of Katherine Short serves as a stark reminder that the pancreas, while small, remains one of the most volatile and unforgiving components of the human digestive and endocrine systems. Immediate clinical evaluation of abdominal distress is not an overreaction; it is a baseline survival requirement.



